Split‐filter DECT improves tumour visibility for radiotherapy planning
21 Sep 2018 Tami Freeman

Pancreatic adenocarcinoma typically has a poor prognosis, and while surgery can cure some cases, 80% of patients with pancreatic cancer are not surgical candidates. Radiation therapy offers an alternative treatment option, but contrast between pancreatic tumours and surrounding healthy tissue is low, making target delineation and treatment planning a challenge.
To address this challenge, a team from the University of Wisconsin-Madison has investigated the ability of split‐filter dual‐energy CT (DECT) to improve pancreatic tumour contrast and contrast‐to‐noise ratio (CNR) for radiotherapy planning. The researchers used the new TwinBeam modality on the SOMATOM Definition Edge CT scanner to image 20 patients with pancreatic adenocarcinoma (J. Appl. Clin. Med. Phys. 19 676).
DECT uses two different photon energies to image patient anatomy, enabling differentiation of tissues with similar density but different composition. TwinBeam utilizes a split‐filter to spatially separate a helical 120 kVp X‐ray beam into a low‐ and a high‐energy beam. Scans can be reconstructed as mixed 120 kVp‐equivalent images, which mimic conventional single‐energy images, or as virtual monoenergetic images (VMIs) with energies ranging from 40 to 190 keV.
Each patient in the study was injected with the iodine contrast OMNIPAQUE, and all but one underwent both pancreatic and portal venous phase scans. For each phase, the researchers reconstructed the raw data using two methods: filtered back projection (FBP) and an iterative reconstruction algorithm called ADMIRE.
To determine the energy that produced the greatest contrast and CNR, the researchers first reconstructed VMIs at 5 keV increments. They found that the 40 keV VMI produced the greatest CNR for pancreatic tumours and used this energy for further studies, along with the VMI at 57 keV, which was chosen based on physician initial preference.
Image analysis
To assess differences in contrast and CNR between the reconstructed datasets, the researchers defined three regions-of-interest (ROIs): the gross tumour volume (GTV); an ROI within healthy pancreatic tissue near the GTV; and an ROI in the erector spinae muscle to assess image noise.
The mean GTV contrast for pancreatic phase images reconstructed using FBP was 15.9 HU for mixed 120 kVp‐equivalent images, 40.7 HU for 57 keV VMIs and 93.7 HU for 40 keV VMIs. For FBP-reconstructed portal venous phase images, the mean GTV contrast was 6.01, 16.4 and 41.5 HU, for the mixed 120 kVp‐equivalent images, 57 keV VMIs and 40 keV VMIs, respectively.
The authors note that, on average, images reconstructed with ADMIRE had slightly greater contrast, but that the improvement was not statistically significant.
Noise in the VMIs increased with decreasing energy, as expected. Averaged over the pancreatic and portal venous phase datasets (which exhibited similar noise levels), the mean image noise was 13.2 HU for mixed 120 kVp‐equivalent images, 20.3 HU for 57 keV VMIs and 28.0 HU for 40 keV VMIs. The use of ADMIRE iterative reconstruction reduced noise to 10.6, 15.8 and 22.2 HU for the respective images — a decrease of about 20% throughout.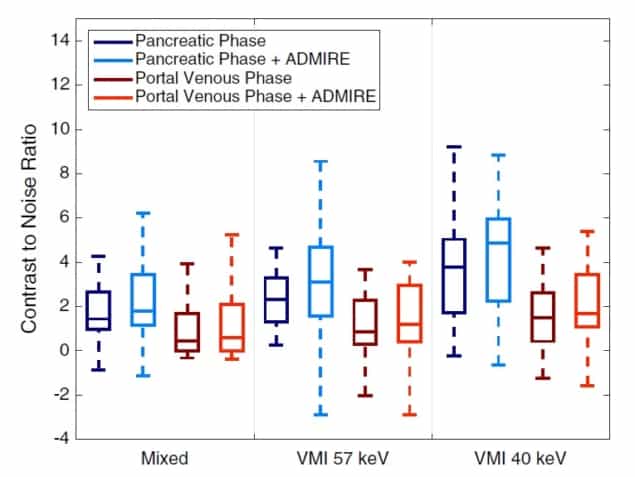 Contrast‐to‐noise ratio for pancreatic and portal venous phase scans, reconstructed with FBP or ADMIRE. (Courtesy: L D Di Maso et al/CC BY 4.0)
Contrast‐to‐noise ratio for pancreatic and portal venous phase scans, reconstructed with FBP or ADMIRE. (Courtesy: L D Di Maso et al/CC BY 4.0)
 Contrast‐to‐noise ratio for pancreatic and portal venous phase scans, reconstructed with FBP or ADMIRE. (Courtesy: L D Di Maso et al/CC BY 4.0)
Contrast‐to‐noise ratio for pancreatic and portal venous phase scans, reconstructed with FBP or ADMIRE. (Courtesy: L D Di Maso et al/CC BY 4.0)
Finally, the researchers calculated the CNR for the six datasets. The mean CNR in the GTV for pancreatic phase images reconstructed with FBP was 1.37, 2.41 and 3.86, for mixed 120 kVp‐equivalent images, 57 keV VMIs and 40 keV VMIs, respectively. ADMIRE further improved the CNR for all cases, increasing to 4.94 in the 40 keV VMIs.
They note that DECT images acquired in the pancreatic phase demonstrated greater GTV contrast and CNR than those acquired during the portal venous phase, suggesting that the pancreatic phase is superior for tumour delineation.
The authors conclude that VMIs reconstructed using split‐filter DECT significantly improved pancreatic tumour contrast and CNR compared with virtual single‐energy CT images, and that iterative reconstruction further improved CNR. This contrast gain may lead to more accurate tumour delineation for radiotherapy planning, potentially leading to more effective treatment.
21/9/2018 FROM PHYSICSWORLD.COM
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου